
Translate this page into:
Migration of Bullet through an Uninjured Gastrointestinal Tract: A Rare Case Report
Corresponding author: Shubhajeet Roy, Faculty of Medical Sciences, King George’s Medical University, Lucknow, India shubhajeet5944.19@kgmcindia.edu
-
Received: ,
Accepted: ,
Abstract
Gunshot injuries are a common case of trauma. We present a rare case of gastrointestinal bullet embolism, in which the bullet had entered the oral cavity via a cheek wound on the right side and was swallowed, following which it migrated and got lodged in the caecum. X-ray was suggestive of presence of a foreign body in the abdomen, whereas FAST (Focussed Assessment with Sonography in Trauma) was negative. CT (Computerised Tomography) was indicative of swallowing the bullet. Colonoscopic removal of the bullet was planned, but there was spontaneous removal of the bullet through faeces, which occurred even before the procedure could be carried out. Following debridement of the laceration and closure of the orocutaneous fistula, the wounds were managed conservatively. Most of the available literature reports cases of intravascular embolization, but the presentation in our case is very rare and not much literature could be found.
Keywords
Bullet
Orocutaneous fistula
colonoscopic removal
facial nerve palsy
INTRODUCTION
Gunshot violence is a never-ending tale of a cataclysm after cataclysm. It is a constant tragedy that urban society faces these days. We present the case of a gastrointestinal bullet embolism, where a bullet had entered the oral cavity through the cheek wound and was swallowed from there into the Gastrointestinal tract and migrated distally, eventually getting lodged in the caecum with no signs and symptoms of injury to the bowel of the patient. This was followed by the spontaneous expulsion of the bullet in the faecal matter by normal peristalsis. The rarity of this condition is the reason behind its dearth of literature.
CASE PRESENTATION
A 32-year-old male presented with a penetrating firearm injury on the right cheek (Figure 1) and difficulty in opening the mouth. On examination, the patient’s vitals were normal with the patient being well oriented to time, place, and person, (Glasgow Coma Scale (GCS) Score was E4V5M6). The wound was lacerated, had poor hygiene, and was spanning approximately 4X3 cm2 from the right ear lobule to the angle of the mandible with flaws over the right ear lobule. The patient presented with no history of respiratory distress or change in voice, or any abnormal breath sounds or emphysema.

- Entry point of wound.
Upper gastrointestinal endoscopy was performed pertaining to the history of dysphagia, which revealed no significant abnormality other than mild fundal gastritis. The patient was evaluated clinico-radiologically and a fracture was noted in the base of the coronoid process of the right ramus of the mandible with loss of alignment of the right temporomandibular joint with grade III facial nerve palsy (Lower Motor Neuron palsy) (Figure 2). There was no other cranial nerve palsy, and nor were any other motor or sensory deficits noted. Also, all four limbs showed normal movements and normal responses to any kind of stimuli. Ophthalmologic examination revealed an inability to close the right eye, photophobia was present, and no history of ocular surgery was reported. X-ray of the pelvis showed a foreign body shadow in the abdomen and focussed assessment with sonography in trauma (FAST) was negative.
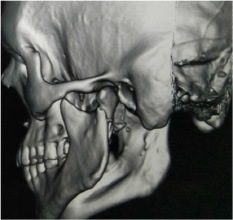
- CT of face– 3D reconstruction showing fracture in the head of the mandible (right side).
No evidence of the bullet was found in the head and neck region, which indicated the formation of an orocutaneous fistula which was confirmed by computerised tomography (CT) scan suggestive of spontaneous swallowing of the bullet in the gastrointestinal tract. A well-defined hyperdensity showed streak artefacts i.e., a foreign body was noted in the abdomen in the right lumbar region, just posterior to the right kidney in the retroperitoneal space, which was suggestive of the lodgement of the bullet in the ascending colon (Figures 3&4).

- X-Ray showing the position of lodgement of bullet in the Ascending Colon.
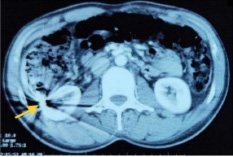
- CT showing the Intra-abdominal position of lodgement of the bullet in the right lumbar region just posterior to the right kidney in the retroperitoneal space.
The patient was scheduled for colonoscopic removal of the bullet from the ascending colon, but there was spontaneous removal of the bullet through faeces before the procedure, the following day. The patient was managed conservatively following debridement of the laceration and closure of the orocutaneous fistula. With his vitals stable and bowel movements normal, he was discharged, and the bullet was handed over to the medico-legal department.
DISCUSSION
The present case of gastrointestinal bullet embolism with spontaneous deglutition, followed by faecal recovery of the bullet is noteworthy due to its relative singularity. This phenomenon is extremely rare because most of the available literature reports cases of intravascular embolization.1 A case report by Tebbett AM et al. in 2012 described the entry of a bullet via the thoracic cavity in a 6-year-old child, which passed in faeces, 5 days after the shooting incidence by normal peristalsis.2 Another case of spontaneous expulsion per rectum was reported by Navsaria P et al. in 2002, wherein the bullet entered the colon through the extraperitoneal space and spontaneously moved out of the body per rectum without requiring any surgical exploration.3 Krispin et al. in 2010 reported a case of post-mortem retrieval of a bullet from the sigmoid colon of a gunshot victim, who died after sustaining 3 gunshot wounds to the abdomen.4 There have been reports of cases involving lodgement of the migrated bullet into the gastrointestinal tract, with or without the clinical evidence of sepsis or intraperitoneal injuries.5 There is evidence of other types of bullet emboli that have also been published such as urethral obstruction due to projectile being retained in the genitourinary system.6 and a case describing acute urinary retention due to late passage of the bullet through the urinary system.7,8 In another case, a bullet had caused esophageal injury and got lodged into the stomach.9 Duhaime OR et al. in 2021 reported a case of retrograde migration of a bullet from the stomach to the oesophagus.10 Another case series described two cases of bullets being expelled through the oral orifice. One case was of a spent bullet from an entry point in the back of the head, which was recovered from the oral orifice, while the other case was of a missile that entered from the chest wall and halted within the lungs and was coughed up by the victim.11 Morrow et al. in 1978 reported the need to consider the possibility of an uneventful passage of a bullet through the gastrointestinal tract.12 Vascular embolization is not uncommon. One review found 46 cases of vascular bullet embolization to be reported within a span of 10 years.1 Clinical signs such as sudden loss of peripheral pulse, unexpected peripheral ischemia, and the sudden onset of new neurological symptoms are presented in case of vascular emboli1 while the only clinical sign of the presenting case was the lack of an exit wound and discovery of an orocutaneous fistula on examination. An effective clinical judgement and radiological imaging enlightened the atypical course of the bullet and supported the clinical diagnosis.
CONCLUSIONS
Intestinal bullet embolism is a rare condition and seldom witnessed by accident and medical emergency teams. Our case of the spontaneous expulsion of the bullet in feces by normal peristalsis preceded by migration of the bullet throughout the gastrointestinal tract from the oral cavity to the anal canal, without causing any additional injuries to the tract is the only known case in the literature. This case highlights the importance of radiological imaging in determining the trajectory of the wandering bullet, and also that of ruling out additional injuries caused by a mobile bullet through endoscopy. A thorough meticulous search via imaging and addressing of resultant damage is a must to account for the missing projectile. This case reminds clinicians to be apprehensive and highly diligent in the evaluation of patients with gunshot wounds.
END NOTE
Author Information
Shubhajeet Roy, Faculty of Medical Sciences, King George’s Medical University, Lucknow, India Devanshi Katiyar, Faculty of Medical Sciences, King George’s Medical University, Lucknow, India Siddhant Aggarwal, Faculty of Medical Sciences, King George’s Medical University, Lucknow, India Jay Tewari, Faculty of Medical Sciences, King George’s Medical University, Lucknow, India Yadvendra Dheer, MCh, Associate Professor, Department of Trauma Surgery, King George’s Medical University, Lucknow, India
Conflict of Interest
None declared
References
- Abdominal shotgun wound with pellet embolization leading to bilateral lower limb amputation: case report and review of the literature of missile emboli over the past 10 years. J Trauma. 2009;67(6):E202-8.
- [CrossRef] [Google Scholar]
- Child road traffic crash injuries at the Red Cross War Memorial Children’s Hospital in Cape Town, South Africa in 1992, 2002 and 2012. Int J Inj Contr Saf Promot. 2015;22(4):352-8.
- [CrossRef] [Google Scholar]
- Spontaneous expulsion of an intracolonic missile after penetrating trauma: a case report. J Trauma. 2002;53(3):586-7.
- [CrossRef] [Google Scholar]
- An Elusive Bullet in the Gastrointestinal Tract: A Rare Case of Bullet Embolism in the Gastrointestinal Tract and a Review of Relevant Literature. Case Rep Crit Care. 2014;2014:1-8.
- [CrossRef] [Google Scholar]
- Urethral obstruction due to the passage of a retained projectile into the genitounrinary system. Am J Emerg Med. 2008;26(7):842-e1-2.
- [CrossRef] [Google Scholar]
- Late migration of a retained bullet into the urinary bladder presenting with acute urinary retention. Isr Med Assoc J. 2007;9(6):484-5.
- [Google Scholar]
- Acute urinary retention from urethral migration of a retained bullet. J Trauma. 2002;53(4):790-2.
- [CrossRef] [Google Scholar]
- Case Report:Emesis of an enteral bullet: A rare case of bullet embolism to the thoracic esophagus. Trauma Case Rep. 2021;34:1-3.
- [CrossRef] [Google Scholar]
- Bullet Emboli in Gunshot Wounds: Practical Aspects of Firearms, Ballistics, and Forensic Techniques CRC Press; 1999.
- [Google Scholar]




